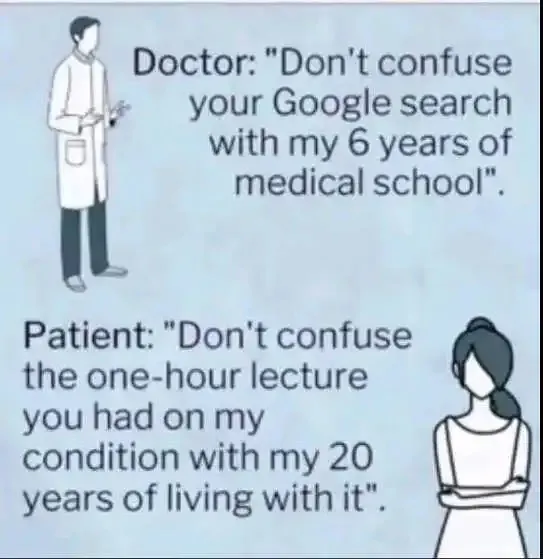
Must be a Brit meme (MBBS programs are often 6 years). In the States, if you spent six years in med school (a four-year program) you’re a retard.
Rant incoming:
Also, anyone not just an asshole with a degree knows that you barely learn shit in med school (Krebs cycle, gimme a fucking break). You learn a FEW things in residency, and a few more things if you do fellowship afterwards, but you still don’t know what you’re doing until you’re a few years out of training and been practicing.
Yeah, I know, just a meme. But I purely despise doctors who think like that arrogant asshole in the meme. (Yeah, THINK. Some can talk all smooth to your face, but still be an arrogant prick inside. Fuck those guys too. In fact, fuck ‘em harder. At least it’s easy to see the openly arrogant ones coming.)
/ENDRANT
Now, equate that to what nurses sometimes(most time) have to contend with… I believe I could have worked with you Mike. I too figured it was a UK meme by the timeline.
It’s been my experience (and I’ve been spending way too much time with them over the last 5 years), that nurses know much more than doctors.
Whenever I see a doctor, I reflexively look over at the nurse and ask “what do you think?”
Nope, wrong.
How so? Show your work.
Says the doctor.
My experience, nothing else. I’ve had three situations over the last couple of years where nurses corrected doctors in front of me about medication issues.
20 or so years ago, I would have said her ass should be fired yesterday (and the individual riding it), but, with the MDs (and whatever other degrees they’ve received from their institutions) from abroad (as well as the broads who “know” they’re better than any MD with aa penis), plus the black MDs who never made it out of high school (Pardon! my racism may be peeking out from behind the hospital corner), she just may have been better educated than the attending.
My only bitch is this:
take yer big f**kin’ mouth into the corridor and suggest to the attending that they (yes, I know! wrong pronoun, but…) reconsider… or possibly she should apply for med school – I’ve known a few that’ve done so.
BTW: only one (out of ~15 or so) nurse during my last hospital excursion (broken ribs) had any more than the slightest acquaintance with the English language; I won’t even discuss their “nursing” skills; in my estimation they were poor to non-existent.
You don’t know how many times I have had to correct and redirect and pull by their nose into NOT KILLING their patient.
“I purely despise doctors who think like that arrogant asshole in the meme”
They’re ALL like that, especially the stupid ones.
TRUTH.
Yup!
It’s the Emm-Diety complex.
MDs are not “better” than nurses. Nor are nurses better than doctors. We have different roles. Think of it as officer and enlisted (NCOs in the case of nurses, and especially for ICU nurses, more like SNCOs). My job as the doctor is not necessarily to know the details (though I should try to know as much as possible). My job is to keep track of the big picture, and to make the overall plan for treatment. The nurse’s role is much more direct patient care, to know the details, to keep me updated in a reasonable timescale, and to tell me when my assumptions about how the patient is doing are wrong. Basically to tell me when I’m fucking up out of ignorance of the details. But that should be done politely, professionally, and ideally not in front of the patient. (Not to protect my pwecious widdle ego, but because the patient doesn’t benefit from having to worry that his doctor is a moron.) In the same vein, I try very very hard to do the same for my nurses, to never undercut them in front of patients or family. If one of us makes the other look bad in public, we are fucking up professionally. And probably personally too, for that matter.
As to skills and knowledge, again, overlapping but DIFFERENT skill sets and responsibilities. An example from my own life as a cancer patient. Rich the nurse (one guy out of many excellent oncology nurses) was way better at all kinds of care stuff, from doing certain procedures to predicting when a patient would have a bad reaction (like shitting themselves after certain drugs) to something. Because he spent 10h daily taking obsessively good care of us inpatients. I’d trust Rich to do certain things over my oncologist (the MD). But my oncologist had to be one to make the treatment plan (what drugs, how many cycles, etc), because she was damn smart, understood the latest treatments, AND the science behind them. After all, her four years of med school, three years of internal medicine residency, and three (I think, not sure about onc) years of oncology fellowship, and 20 years of practice are good for SOMETHING. But neither was “better”. Different roles.
In my own role, yeah, I can put in an IV. But you might not like the experience, because I hardly ever did that. You’d have a MUCH better experience if, say, Kevin put in your IV (trust me on this). But I know how to do cardiac catheterization, for example, which he probably doesn’t do.
I know how to scan, how to do an echocardiogram, but you’d get a much better study if my lead tech Angela did it. When it comes to “reading” the echoes (cardiac ultrasound), Angela and I both have “good eyes”. I’ll admit that sometimes she sees stuff that I don’t. But I have a better idea of what the findings mean, and what the treatment (if any) should be, and the alternative treatments, and the side effects and whether there’s interaction with the patient’s OTHER medical problems. Finally, while we don’t check with each other on every damn thing, on big picture stuff (this is more about protocols rather than individual patient care), I’ll definitely ask for input from not just Angela, but our other techs too. This is not a cowardly bullshit thing of trying to push my responsibilities on those “under” me, but because they’re smart people who may have noticed stuff I don’t even know about. Or they see potential problems in certain details that I don’t see as problems because I don’t do that stuff directly (often at least). And it’s important for the team to feel “heard”. But ultimately I have to put my dime down and make the final decision. (Also, I have people above me who also get their input… but if it’s a problem at my level I need to be a big boy and just handle it. Just like any other job.)
Long non-rant. But I’m at the airport waiting for my flight and don’t want to read the papers I told myself I’d read.
Thank you Mike, hearing it from the source. I always felt like a JR partner to the attending. I respected his role and the burden of responsibility for carrying the water, his shoulders so to speak. It took a lot of education, training and continuous education on my part and a developed skill set to be his adjunct. I did well enough I had doctors come to me for consultation and advice as I developed into a good diagnostician in my own layman way, doing so was constant study, being very observant and remaining professional and consistent. I became a nurse when doctors and nurses had more leeway into thinking outside the box, consider alternative therapies and procedures.
Dr. Mike_C, how eloquently stated! You hit the nail on the head, mutual respect if due. As a cardiac nurse, I would have LOVED to have worked with a doctor of your caliber and professionalism. Much respect. Blessings to you dear sir.

Must be a Brit meme (MBBS programs are often 6 years). In the States, if you spent six years in med school (a four-year program) you’re a retard.
Rant incoming:
Also, anyone not just an asshole with a degree knows that you barely learn shit in med school (Krebs cycle, gimme a fucking break). You learn a FEW things in residency, and a few more things if you do fellowship afterwards, but you still don’t know what you’re doing until you’re a few years out of training and been practicing.
Yeah, I know, just a meme. But I purely despise doctors who think like that arrogant asshole in the meme. (Yeah, THINK. Some can talk all smooth to your face, but still be an arrogant prick inside. Fuck those guys too. In fact, fuck ‘em harder. At least it’s easy to see the openly arrogant ones coming.)
/ENDRANT
Now, equate that to what nurses sometimes(most time) have to contend with… I believe I could have worked with you Mike. I too figured it was a UK meme by the timeline.
It’s been my experience (and I’ve been spending way too much time with them over the last 5 years), that nurses know much more than doctors.
Whenever I see a doctor, I reflexively look over at the nurse and ask “what do you think?”
Nope, wrong.
How so? Show your work.
Says the doctor.
My experience, nothing else. I’ve had three situations over the last couple of years where nurses corrected doctors in front of me about medication issues.
20 or so years ago, I would have said her ass should be fired yesterday (and the individual riding it), but, with the MDs (and whatever other degrees they’ve received from their institutions) from abroad (as well as the broads who “know” they’re better than any MD with aa penis), plus the black MDs who never made it out of high school (Pardon! my racism may be peeking out from behind the hospital corner), she just may have been better educated than the attending.
My only bitch is this:
take yer big f**kin’ mouth into the corridor and suggest to the attending that they (yes, I know! wrong pronoun, but…) reconsider… or possibly she should apply for med school – I’ve known a few that’ve done so.
BTW: only one (out of ~15 or so) nurse during my last hospital excursion (broken ribs) had any more than the slightest acquaintance with the English language; I won’t even discuss their “nursing” skills; in my estimation they were poor to non-existent.
You don’t know how many times I have had to correct and redirect and pull by their nose into NOT KILLING their patient.
“I purely despise doctors who think like that arrogant asshole in the meme”
They’re ALL like that, especially the stupid ones.
TRUTH.
Yup!
It’s the Emm-Diety complex.
MDs are not “better” than nurses. Nor are nurses better than doctors. We have different roles. Think of it as officer and enlisted (NCOs in the case of nurses, and especially for ICU nurses, more like SNCOs). My job as the doctor is not necessarily to know the details (though I should try to know as much as possible). My job is to keep track of the big picture, and to make the overall plan for treatment. The nurse’s role is much more direct patient care, to know the details, to keep me updated in a reasonable timescale, and to tell me when my assumptions about how the patient is doing are wrong. Basically to tell me when I’m fucking up out of ignorance of the details. But that should be done politely, professionally, and ideally not in front of the patient. (Not to protect my pwecious widdle ego, but because the patient doesn’t benefit from having to worry that his doctor is a moron.) In the same vein, I try very very hard to do the same for my nurses, to never undercut them in front of patients or family. If one of us makes the other look bad in public, we are fucking up professionally. And probably personally too, for that matter.
As to skills and knowledge, again, overlapping but DIFFERENT skill sets and responsibilities. An example from my own life as a cancer patient. Rich the nurse (one guy out of many excellent oncology nurses) was way better at all kinds of care stuff, from doing certain procedures to predicting when a patient would have a bad reaction (like shitting themselves after certain drugs) to something. Because he spent 10h daily taking obsessively good care of us inpatients. I’d trust Rich to do certain things over my oncologist (the MD). But my oncologist had to be one to make the treatment plan (what drugs, how many cycles, etc), because she was damn smart, understood the latest treatments, AND the science behind them. After all, her four years of med school, three years of internal medicine residency, and three (I think, not sure about onc) years of oncology fellowship, and 20 years of practice are good for SOMETHING. But neither was “better”. Different roles.
In my own role, yeah, I can put in an IV. But you might not like the experience, because I hardly ever did that. You’d have a MUCH better experience if, say, Kevin put in your IV (trust me on this). But I know how to do cardiac catheterization, for example, which he probably doesn’t do.
I know how to scan, how to do an echocardiogram, but you’d get a much better study if my lead tech Angela did it. When it comes to “reading” the echoes (cardiac ultrasound), Angela and I both have “good eyes”. I’ll admit that sometimes she sees stuff that I don’t. But I have a better idea of what the findings mean, and what the treatment (if any) should be, and the alternative treatments, and the side effects and whether there’s interaction with the patient’s OTHER medical problems. Finally, while we don’t check with each other on every damn thing, on big picture stuff (this is more about protocols rather than individual patient care), I’ll definitely ask for input from not just Angela, but our other techs too. This is not a cowardly bullshit thing of trying to push my responsibilities on those “under” me, but because they’re smart people who may have noticed stuff I don’t even know about. Or they see potential problems in certain details that I don’t see as problems because I don’t do that stuff directly (often at least). And it’s important for the team to feel “heard”. But ultimately I have to put my dime down and make the final decision. (Also, I have people above me who also get their input… but if it’s a problem at my level I need to be a big boy and just handle it. Just like any other job.)
Long non-rant. But I’m at the airport waiting for my flight and don’t want to read the papers I told myself I’d read.
Thank you Mike, hearing it from the source. I always felt like a JR partner to the attending. I respected his role and the burden of responsibility for carrying the water, his shoulders so to speak. It took a lot of education, training and continuous education on my part and a developed skill set to be his adjunct. I did well enough I had doctors come to me for consultation and advice as I developed into a good diagnostician in my own layman way, doing so was constant study, being very observant and remaining professional and consistent. I became a nurse when doctors and nurses had more leeway into thinking outside the box, consider alternative therapies and procedures.
Dr. Mike_C, how eloquently stated! You hit the nail on the head, mutual respect if due. As a cardiac nurse, I would have LOVED to have worked with a doctor of your caliber and professionalism. Much respect. Blessings to you dear sir.